Content
A Class S autoclave is a steam sterilizer designed to handle a specific, manufacturer-defined range of loads — sitting between the basic Class N and the fully capable Class B in terms of sterilization performance. In dental practice, the Class S autoclave is one of the most commonly used sterilization units, because it offers a practical balance between cost, cycle speed, and the ability to process hollow and porous instruments that are standard in any dental clinic.
The classification system comes from the European standard EN 13060, which divides small steam sterilizers into three classes — N, S, and B — based on their steam penetration capability and the types of loads they can safely sterilize. Understanding which class your autoclave belongs to is not just a regulatory checkbox; it directly determines whether your instruments are being fully sterilized or merely surface-treated.
For most dental practices, the critical question is whether a Class S dental autoclave can handle the full range of instruments used — from solid metal tools to hollow handpieces, bagged pouches, and porous wrapped loads. The answer depends on the specific sub-cycles the manufacturer has validated for that machine, which is exactly what makes Class S a nuanced category rather than a fixed standard.
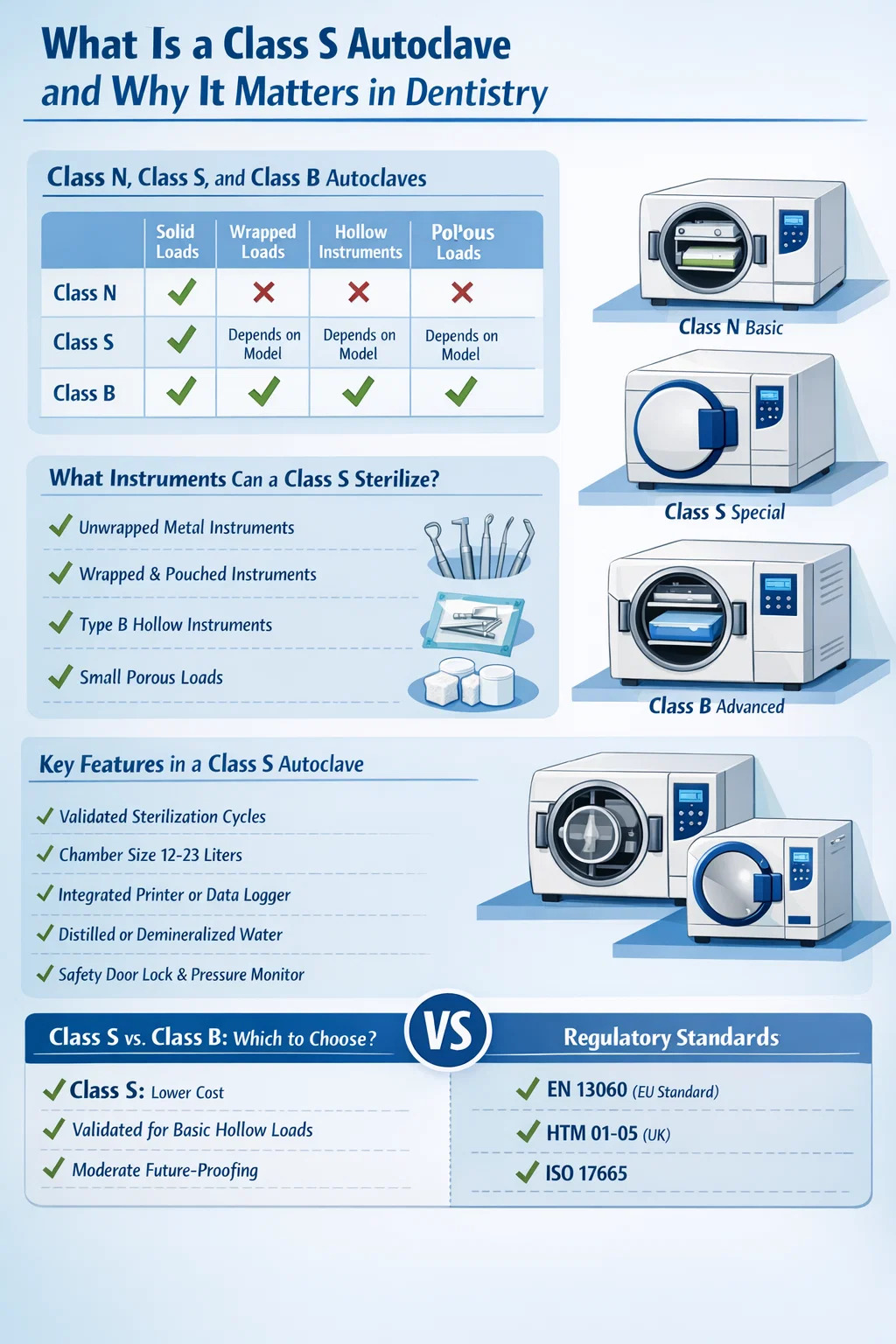
Before going deeper into Class S, it helps to understand how the three classifications differ in practical terms. The EN 13060 standard defines them clearly, and each has a specific scope of application.
| Autoclave Class | Solid Unwrapped Loads | Wrapped/Pouched Loads | Hollow Instruments (Type B) | Porous Loads |
|---|---|---|---|---|
| Class N | YS | NO | NO | NO |
| Class S | YS | Depends on model | Depends on model | Depends on model |
| Class B | YS | YS | YS | YS |
Class N (where "N" stands for Naked) sterilizes only solid, unwrapped instruments. It uses a gravity displacement steam process and cannot guarantee steam penetration into cavities, wrapped pouches, or porous materials. It is the most limited option and generally unsuitable for comprehensive dental instrument sterilization.
Class B (where "B" stands for Big or Universal) uses a pre-vacuum cycle — typically a fractionated vacuum or pulsed vacuum process — to actively remove air from the chamber before steam enters. This ensures steam penetration into hollow lumens, wrapped loads, and porous materials. Class B is the gold standard for dental sterilization and is required by many national health authorities for processing dental handpieces.
Class S (where "S" stands for Special) occupies a defined but flexible middle ground. The manufacturer specifies exactly which load types the machine has been validated for. A Class S dental autoclave may be capable of sterilizing bagged instruments and some hollow loads, but only if the manufacturer has tested and documented those cycles. This means two Class S autoclaves from different brands can have significantly different capabilities.
All autoclaves, regardless of class, rely on saturated steam under pressure to destroy microbial life. The basic principle is straightforward: steam at elevated temperatures — typically 134°C (273°F) at approximately 2 bar of pressure — denatures proteins in bacteria, viruses, spores, and fungi, killing them within a defined holding time. At 134°C, the standard holding time is 3 to 18 minutes depending on the load type and cycle design. At the lower temperature of 121°C, the holding time extends to around 15 to 30 minutes.
What separates Class S from Class N is the air removal method used before steam enters the chamber. Air is a poor conductor of heat compared to steam and, if trapped, creates cool spots that prevent sterilization. Class N machines rely on gravity displacement — steam pushes air out through a drain at the bottom of the chamber. This works for simple solid loads but fails with complex geometries.
Class S autoclaves typically use one or more of the following air removal approaches, depending on the specific model and its validated load types:
After sterilization, the drying phase is equally important in a dental context. Instruments that exit the autoclave wet can be recontaminated through capillary action in pouches or through handling. Class S dental autoclaves designed for bagged loads must include an effective drying cycle — typically a post-vacuum drying phase — to ensure instruments remain sterile until use.
This is the most practical question for any dental clinic evaluating a Class S autoclave, and the answer requires reading the manufacturer's validated load specifications rather than relying on the class label alone. That said, most Class S dental autoclaves on the market today are designed to handle at least the following:
Metal instruments such as forceps, mirrors, explorers, scalers, and similar solid tools are the easiest load for any autoclave. Class S handles these without difficulty, and for practices that use instruments immediately after sterilization — without long-term storage — this cycle alone may be sufficient for part of the instrument inventory.
Most Class S dental autoclaves validate pouched loads — instruments sealed in sterilization pouches or wrapped in sterilization paper — because this is a fundamental requirement for maintaining sterility between sterilization and use. Steam penetration through the pouch material requires more than gravity displacement, which is why Class S typically employs SFPP or pre-vacuum cycles for this purpose. Always verify that the specific Class S unit has been validated for pouched loads before purchasing.
This is where Class S becomes more complex. EN 13060 defines two types of hollow loads:
For dental handpiece sterilization specifically, regulatory bodies in multiple countries — including the UK's Department of Health and Australia's National Health and Medical Research Council — recommend or require Class B autoclaves. A Class S autoclave can only be used for handpieces if it is explicitly validated for Type A hollow loads, and such validation must be documented.
Gauze, cotton rolls, and similar textiles are porous loads. Some Class S autoclaves are validated for small quantities of porous material, though full porous load capability is more commonly associated with Class B. In most dental settings, porous loads are single-use disposables, so this is less of a practical concern.
Not all Class S dental autoclaves are equal. When evaluating models for a dental practice, these are the features that determine real-world performance and compliance:
Dental autoclaves are available in chamber sizes ranging from as small as 6 liters to around 23 liters for tabletop units. Common sizes for single-surgery dental practices are 12 to 18 liters, which can accommodate two to four trays of instruments per cycle. Larger multi-surgery practices often opt for 22-liter or larger units, or multiple smaller units running in parallel to keep up with patient throughput.
Chamber volume directly affects cycle time per instrument set. A smaller chamber that fills faster may turn instruments around more quickly for a single surgery, while a larger chamber processes more instruments per run. Matching chamber size to the actual daily instrument volume prevents the inefficiency of running many small cycles or, worse, overloading the chamber.
A well-specified Class S dental autoclave should offer at minimum the following cycles:
Some Class S dental autoclaves also include a handpiece-specific cycle if the unit has been validated for Type A hollow loads, as well as a test cycle for Bowie-Dick or helix testing.
Cycle documentation is a regulatory requirement in most countries. Each sterilization cycle must be recorded with the date, time, cycle parameters, and a pass/fail result. Many Class S dental autoclaves include an integrated thermal printer, while others connect via USB or network to external logging software. Digital logging with tamper-evident records is becoming the preferred standard, as it allows for easy auditing and traceability — particularly important for practices that process instruments for multiple patients per day.
Autoclaves are sensitive to water quality. Using tap water with high mineral content leads to scale buildup on heating elements and chamber walls, shortens the service life of the unit, and can contaminate instruments. Most manufacturers require — and EN 13060 specifies — the use of distilled or demineralized water with a conductivity of no more than 15 µS/cm. Some Class S dental autoclaves include a built-in water treatment system or reservoir monitoring; others require the operator to supply pre-treated water externally.
Autoclave chambers operate under pressure. Door locking mechanisms must prevent opening during active cycles. High-quality Class S dental autoclaves use electronic door locks with pressure interlocks — the door cannot be opened if pressure is above ambient. Additional safety features include pressure relief valves, over-temperature cutoffs, and water level sensors. These are not optional extras; they are basic safety requirements that should be confirmed before purchase.
Total cycle time — from door close to dry instruments ready for use — varies significantly between models. A fast Class S dental autoclave completes a wrapped instrument cycle in as little as 30 minutes, while slower units may take 45 to 60 minutes for the same load. In a busy dental practice where instrument sets need to be turned around between patients, cycle time is a direct operational variable that affects how many instrument sets the practice needs to own and how efficiently the sterilization room runs.
Sterilization in dental practice is governed by a combination of international standards, national regulations, and professional guidelines. Understanding the regulatory landscape helps practices choose the right autoclave class and maintain compliant processes.
EN 13060 is the European standard that defines the performance requirements for small steam sterilizers — those with chambers of 60 liters or less. It establishes the N, S, and B classification system, defines the test methods for validating each class, and specifies documentation requirements. In Europe, a dental autoclave must carry CE marking and comply with EN 13060 to be legally placed on the market. The standard was first published in 2004 and has been revised since; practices should confirm that their unit complies with the current version.
The UK's Health Technical Memorandum 01-05 ("Decontamination in primary care dental practices") provides detailed guidance on sterilization requirements for UK dental practices. It distinguishes between "essential quality requirements" and "best practice" requirements. HTM 01-05 best practice recommends Class B autoclaves for processing all wrapped and hollow instruments, including dental handpieces. Class S autoclaves are permitted under essential quality requirements for certain load types but may not meet best practice thresholds in all scenarios. Practices operating under NHS contracts in England should familiarize themselves with HTM 01-05 requirements.
ISO 17665 covers the validation and routine control of moist heat sterilization for medical devices — applicable to dental instruments sterilized in autoclaves. ISO 11135 is specific to ethylene oxide sterilization and less relevant in the dental autoclave context. For dental practices, ISO 17665 informs the validation testing that autoclave manufacturers must perform to support their cycle claims. When a manufacturer states that a Class S unit is validated for pouched loads, that validation is expected to follow ISO 17665 methodology.
Owning a Class S dental autoclave is only half the compliance equation. Ongoing testing is required to confirm the unit continues to perform within specification. Standard testing includes:
Many practices underestimate the ongoing maintenance and testing burden associated with autoclave compliance. Factoring in service contracts, consumables (indicators, pouches, printer paper, distilled water), and periodic validation testing gives a more accurate picture of total cost of ownership.
This is the most common decision point for dental practices. The choice depends on the instrument types used, the national regulatory requirements, the budget, and the operational workflow of the practice.
| Factor | Class S Dental Autoclave | Class B Dental Autoclave |
|---|---|---|
| Purchase cost (tabletop) | Generally lower | Generally higher |
| Handpiece sterilization | Only if validated for Type A hollow loads | Yes, standard |
| Wrapped instrument capability | Most models, if validated | All models |
| Regulatory ceiling (UK HTM 01-05) | Essential quality only | Best practice |
| Cycle speed (typical wrapped load) | 30–50 minutes | 25–45 minutes |
| Future-proofing | Moderate | High |
For a dental practice that uses rotary handpieces — which is every practice — Class B is the more defensible choice from a clinical and regulatory standpoint. Handpiece sterilization is a well-documented infection control requirement, and the consequences of inadequate sterilization are serious, both for patient safety and professional liability.
However, a Class S dental autoclave remains a sensible option in specific scenarios: as a secondary unit running alongside a Class B for solid instrument turnaround, in practices with a very limited instrument range that does not include critical hollow loads, or in jurisdictions where Class S meets all applicable regulatory requirements for the specific instruments being processed.
Budget constraints are real, and the cost difference between a basic Class S and a fully specified Class B can range from a few hundred to several thousand euros or pounds depending on the brand and features. That said, autoclave replacements typically occur every 7 to 12 years in a busy practice, making the per-year cost difference relatively modest when amortized across the working life of the unit.
Proper maintenance is not just about protecting the machine — it is a direct factor in sterilization efficacy. An autoclave that is poorly maintained may produce cycles that appear to complete successfully but fail to achieve the required sterility assurance level.
Most manufacturers and regulatory bodies require an annual service by a qualified technician. This typically includes calibration of temperature and pressure sensors, inspection of the safety relief valve, replacement of consumable seals and filters, and a full performance qualification test. Service records should be retained for the working life of the autoclave and made available for regulatory inspection if required.
Even a perfectly maintained Class S dental autoclave can fail to sterilize instruments if they are loaded incorrectly. Common loading errors include:
Indicators are an essential part of using any dental autoclave correctly. They provide evidence that instruments have been exposed to sterilization conditions — but they must be used and interpreted correctly.
Chemical indicators (CIs) change color when exposed to steam at the correct temperature and time. They are classified under ISO 11140-1 into several types:
In daily dental practice, Type 1 indicators on pouches and Type 5 or 6 indicators inside loads provide a practical first line of verification. A failed indicator — one that does not change color correctly — means the load should not be used and the autoclave should be taken out of service for investigation.
Biological indicators (BIs) contain actual bacterial spores — typically Geobacillus stearothermophilus for steam sterilization — which are among the most heat-resistant forms of microbial life. After a sterilization cycle, the BI is incubated for 24 to 48 hours. If no growth occurs, sterilization conditions were sufficient to kill the spores. Biological indicator testing should be performed at least weekly and after any cycle anomaly, autoclave repair, or reinstallation.
A PCD, such as a hollow helix device, simulates a challenging load condition — typically a long narrow lumen — and contains a chemical or biological indicator at its most difficult-to-sterilize point. For Class S dental autoclaves validated for hollow loads, routine helix testing confirms that steam continues to penetrate the device's lumen adequately. A failed helix test is a strong signal that the air removal system or steam quality has degraded.
Understanding common failure modes helps dental teams respond appropriately rather than continuing to use a malfunctioning unit.
| Problem | Likely Cause | Action |
|---|---|---|
| Instruments wet after cycle | Drying phase failure, overloaded chamber, blocked filter | Reduce load, check filter, extend drying, service if persists |
| Cycle abort / pressure not reached | Door seal leak, insufficient water, faulty heating element | Inspect door gasket, check water level, call service engineer |
| Failed chemical indicator | Inadequate temperature or time, air in chamber | Do not use load, quarantine instruments, investigate cause before reuse |
| Unusual cycle time increase | Scale buildup on heating element | Run descaling cycle, check water quality |
| Corrosion on instruments after cycling | Incorrect water quality, incompatible instruments, chamber contamination | Verify distilled water use, check instrument material compatibility |
One consistent rule applies across all failure scenarios: instruments processed in a failed or suspect cycle must be considered non-sterile and must not be used on patients. They should be reprocessed in a verified cycle after the autoclave problem has been diagnosed and corrected.
A point that is sometimes overlooked in discussions of dental autoclave performance is the critical importance of pre-cleaning. Steam sterilization destroys microorganisms, but it cannot substitute for physical removal of bioburden — blood, saliva, tissue debris, and other organic material.
Organic material on instrument surfaces physically blocks steam contact with the underlying metal, preventing sterilization. It can also bake onto instrument surfaces during the heat cycle, making it much harder to remove afterward and potentially protecting microorganisms beneath it. A heavily contaminated instrument placed into an autoclave without prior cleaning is not reliably sterilized regardless of cycle class.
The standard pre-cleaning workflow in a dental setting includes:
Washer-disinfectors, which automate steps 2 through 4, are increasingly common in dental practices and significantly improve cleaning consistency compared to manual methods. They also reduce staff exposure to sharps and contaminated instruments during the cleaning process. Using a validated washer-disinfector as part of the reprocessing chain is considered best practice in many guidelines and strengthens the overall sterility assurance of the dental autoclave process.







If you have any question for the installation
or need support, please feel free to contact us.
86-15728040705
86-18957491906
 English
English عربى
عربى