Content
A dental autoclave is a pressurized sterilization device that uses saturated steam at high temperatures — typically between 121°C and 135°C — to eliminate all forms of microbial life, including bacteria, viruses, fungi, and spores. In a clinical dental setting, it is not optional equipment. It is a regulatory and ethical requirement in virtually every country.
The short answer for any dental professional asking whether they need one: yes, without exception. Reusable instruments — handpieces, scalers, forceps, mirrors, burs — must be sterilized between every patient use. A dentist autoclave is the only method validated to achieve sterility assurance levels (SAL) of 10⁻⁶, meaning the probability of a surviving microorganism is less than one in a million.
Chemical disinfection, UV cabinets, and glass bead sterilizers do not meet the same standard. Infection control bodies — including the CDC, WHO, and national dental associations — consistently point to steam sterilization as the gold standard. Understanding how a dental autoclave works, what types exist, and how to maintain one properly is foundational knowledge for any practice.

The mechanism of a dental autoclave relies on three interdependent variables: temperature, pressure, and time. Steam under pressure reaches temperatures that liquid water cannot achieve at atmospheric levels. At 121°C, standard steam sterilization requires approximately 15 minutes of exposure. At 134°C, the same sterilization can be achieved in as little as 3 to 4 minutes.
The steam itself is the active agent. Moist heat denatures proteins within microbial cells, destroying enzymatic and structural functions irreversibly. Dry heat requires significantly higher temperatures (160°C to 180°C) and longer cycle times to achieve the same result because steam transfers energy far more efficiently than air.
A standard autoclave cycle passes through three phases:
Understanding these phases helps clinicians interpret cycle failures, troubleshoot errors, and make sense of validation logs — all of which are required for regulatory compliance.
The European Standard EN 13060 classifies small steam sterilizers into three types based on their capability to sterilize different load configurations. This classification is widely adopted globally and is the most practical framework for dental practices evaluating equipment options.
| Class | Vacuum System | Suitable For | Typical Use Case |
|---|---|---|---|
| Class B | Pre-vacuum (fractioned) | Wrapped, unwrapped, porous, hollow instruments | Full-service dental clinics, surgical centers |
| Class S | Partial or single vacuum | Specified by manufacturer; often wrapped solid items | Mid-range dental practices with defined load types |
| Class N | No vacuum (gravity displacement) | Unwrapped solid instruments only | Clinics with simple, unwrapped instrument loads |
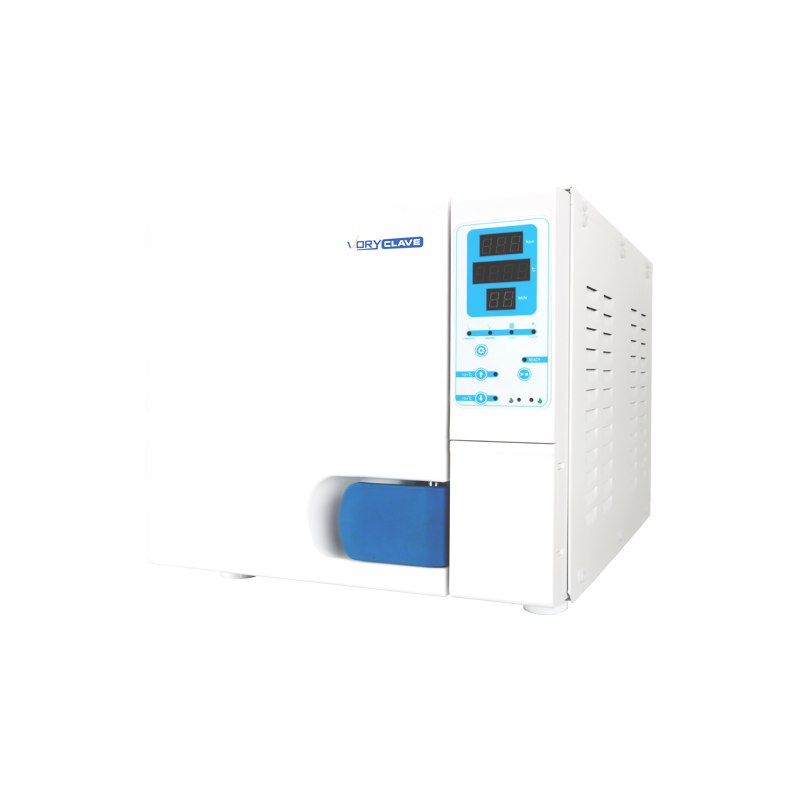
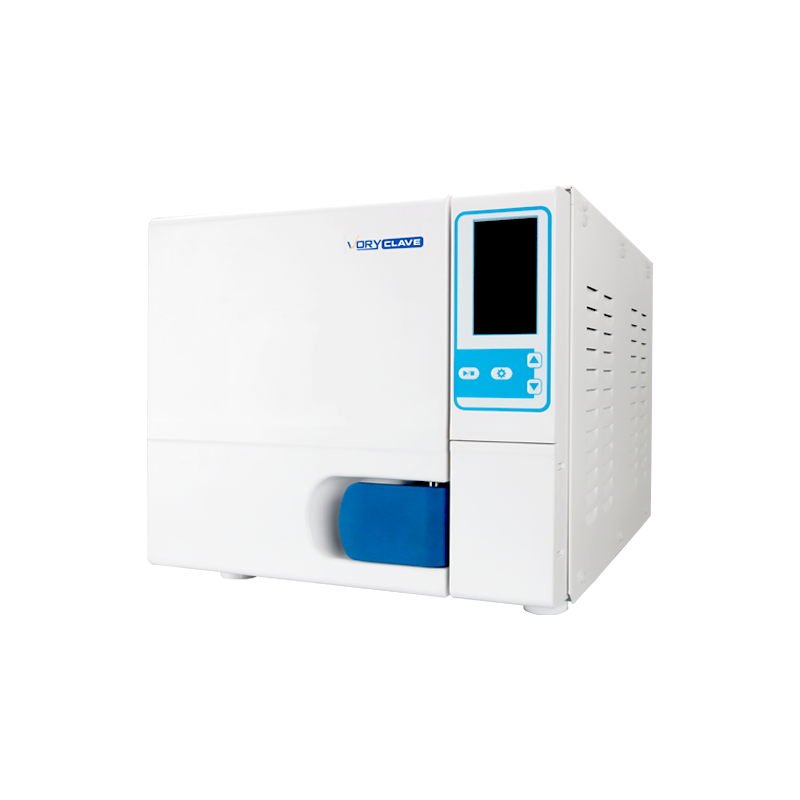
Class B dental autoclaves are considered the benchmark for modern dental practices. The "B" stands for "big small sterilizers," reflecting their broad capability. Fractioned pre-vacuum cycles remove air in multiple pulses before steam admission, ensuring steam penetrates even complex hollow instruments like handpieces, endodontic files within tubes, and implant components packaged in double pouches.
In many European countries, Class B is now the minimum regulatory requirement for sterilizing wrapped instruments. Practices that attempt to use Class N machines for packaged loads are in direct violation of infection control standards — a liability risk that extends beyond regulatory fines to patient harm claims.
Class N machines are the simplest and least expensive option. They work adequately for unwrapped solid metal instruments that will be used immediately after sterilization. However, they cannot reliably sterilize wrapped loads, hollow items, or porous materials. Practices relying on Class N equipment must have strict protocols ensuring instruments are used before recontamination occurs.
Selecting the right autoclave for a dental practice is a purchasing decision with long-term operational and compliance implications. Price alone is a poor selection criterion. The following factors should drive the evaluation process:
Dental autoclave chamber sizes are measured in liters, typically ranging from 8 liters for small countertop units to 23 liters or more for larger clinical models. A busy multi-chair dental practice with six or more operatories and high patient volume needs substantially more capacity than a solo practitioner seeing twenty patients per week.
A common calculation error is buying a unit with adequate volume but failing to account for cycle time. A 17-liter Class B dental autoclave running a full cycle in 30 to 35 minutes can process roughly 12 to 16 full cycles in an 8-hour clinical day — but only if loading, unloading, and documentation time is managed efficiently. Practices processing high volumes of complex loads should consider two smaller units rather than one large unit to avoid a single point of failure.
Wet packs are a persistent clinical headache. Instruments packaged in paper-plastic pouches that exit the autoclave still moist must be re-processed, creating delays and consuming pouches. Models with dedicated forced-air drying or heated drying chambers perform significantly better than those relying on passive residual heat. When evaluating equipment, ask vendors to demonstrate cycle completion on a full load, not just a demonstration load, and inspect the dryness of the pouches directly.
Regulatory bodies in most countries now require practices to maintain sterilization records for a minimum of five to ten years. Modern dental autoclaves connect via USB, Ethernet, or wireless to practice management systems or dedicated logging software. Each cycle should generate a printable or digital record showing date, time, cycle type, temperature achieved, pressure, exposure duration, and pass/fail status.
Traceability systems that link individual sterilization cycles to patient records are increasingly common in surgical and implant dentistry. These systems allow practices to identify which patients received instruments from a failed cycle — critical for incident management.
All dental autoclaves require distilled or deionized water. Tap water, even in regions with soft water supplies, contains minerals that deposit scale on chamber walls, heating elements, and valves. Scale buildup reduces sterilization efficiency, damages equipment, and voids warranties. Practices in areas with hard water should budget for a water purification unit or a reliable distilled water supply. Using demineralized water with a conductivity below 15 µS/cm is the standard recommendation from most manufacturers.
Different instruments require different cycle parameters. Handpieces, particularly those with internal lubricants, may require dedicated cycles that avoid excessive temperature or drying pressure that could degrade internal components. Rubber and silicone items require lower-temperature cycles. Practices investing in a dental autoclave sterilizer should verify that the unit offers at least three to four programmable cycle options, including a rapid cycle for emergency instrument turnaround.
Owning a dental autoclave and running cycles is not sufficient for compliance. Practices must validate that their autoclave is actually achieving sterilization. This involves a layered testing approach using three types of indicators.
Practices should document every BI test result. If a biological indicator fails, the protocol is clear: quarantine all loads processed since the last successful BI test, recall instruments if possible, notify affected patients if instruments were already used clinically, service the autoclave, and run three consecutive successful BI cycles before returning to clinical use.

A dental autoclave is a pressure vessel with heating elements, seals, gaskets, pumps, and control boards. Like all mechanical equipment, it requires systematic maintenance to remain reliable. Neglected autoclaves fail at inconvenient moments, disrupt clinical workflow, and — in the worst case — produce false-positive sterilization results where instruments appear processed but were not adequately treated.
Dental autoclaves must undergo annual preventive maintenance and certification by a qualified technician. This service includes calibration of thermocouples and pressure gauges, replacement of door gaskets and filter elements, inspection of valve function, and confirmation that the unit continues to meet the EN 13060 or equivalent standard for its class. Annual certification records must be retained and available for inspection by regulatory authorities.
Some manufacturers specify more frequent service intervals — every 6 months — for high-throughput units running 15 or more cycles per day. Exceeding recommended service intervals not only increases breakdown risk but may invalidate warranty coverage.
Cycle errors and equipment faults are inevitable over the lifespan of any dental autoclave sterilizer. Knowing how to interpret error codes and identify root causes saves time and prevents unnecessary service calls for issues that can be resolved in-practice.
| Error / Symptom | Common Cause | Recommended Action |
|---|---|---|
| Cycle aborts before completion | Door seal failure, low water level, pressure leak | Inspect gasket, refill water, check door latch mechanism |
| Wet packs after drying cycle | Overloaded chamber, blocked drain filter, inadequate drying time | Reduce load density, clean drain filter, extend drying program |
| Failed Bowie-Dick test | Air in chamber, vacuum pump issue, steam quality problem | Do not use unit; contact service technician immediately |
| Instrument corrosion after sterilization | Tap water used instead of distilled, dissimilar metals in contact | Switch to distilled water, segregate instrument types on trays |
| Staining or discoloration on chamber walls | Mineral scale buildup, debris from unclean instruments | Run a descaling cycle with approved cleaner, improve pre-cleaning of instruments |
| Positive biological indicator result | Equipment malfunction, overloaded chamber, wrong cycle selected | Quarantine all loads, take unit out of service, investigate and re-validate |
Dental handpieces — high-speed turbines, slow-speed contra-angles, and surgical motors — represent one of the most complex sterilization challenges in any dental practice. They have internal hollow channels, lubrication pathways, and turbine bearings that require specific handling to sterilize safely without accelerating mechanical wear.
The CDC and most national infection control guidelines classify dental handpieces as semicritical to critical items depending on use, and require steam sterilization between every patient. This was not always standard practice — historically, external wiping was considered sufficient — but research showing internal contamination of handpiece turbines changed the clinical and regulatory consensus definitively.
Using a Class B dental autoclave is essential for handpiece sterilization. Class N machines using gravity displacement cannot guarantee steam penetration into hollow handpiece turbine channels, making them insufficient for this instrument type regardless of the cycle parameters displayed on the control panel.
Dental autoclaves are regulated medical devices in most jurisdictions. In the European Union, they fall under the Medical Device Regulation (MDR 2017/745). In the United States, the FDA classifies steam sterilizers as Class II medical devices. In Australia, the Therapeutic Goods Administration (TGA) and AS/NZS 4815 govern sterilization in dental settings. Each jurisdiction has specific requirements around purchase, validation, maintenance, and documentation.
When infection control inspectors visit dental practices, sterilization documentation is among the first areas reviewed. Inspectors typically check for:
Practices found non-compliant can face suspension of their operating license, mandatory re-training, and in cases involving patient harm, civil liability. The reputational cost of a publicized infection control failure in a dental practice is typically far greater than the operational investment required to maintain compliance.
The dental autoclave market includes a range of manufacturers with different positioning on price, performance, and after-sales support. While individual product lines change over time, several brands have established long-standing reputations in the dental sector.
When comparing brands, practices should evaluate not just the unit cost but the availability and cost of spare parts, local service technician networks, software update policies, and the manufacturer's track record on firmware-related issues. A cheaper unit with no local service support can become significantly more expensive over a five-year operational period.

Purchase price for a dental autoclave sterilizer varies considerably based on class, chamber size, and brand. Entry-level Class N models start around $1,500 to $3,000 USD. Mid-range Class B units with 17- to 22-liter chambers typically cost between $4,000 and $9,000 USD. Premium Class B models with integrated traceability software and advanced drying systems can reach $12,000 to $18,000 USD or more.
However, the purchase price represents only part of the total cost of ownership. Practices should budget for:
A well-maintained Class B dental autoclave from a reputable brand has a realistic service life of 10 to 15 years. Amortized over that period, even a premium unit represents a modest daily operational cost relative to the clinical risk managed and the regulatory exposure avoided.
A dental autoclave is only as effective as the people operating it. Equipment failure is far less common than human error — incorrect loading, wrong cycle selection, skipped documentation, or failure to act on a failed indicator. Staff training is not a one-time onboarding task. It requires periodic refreshers, competency assessments, and updated training whenever new equipment or protocols are introduced.
Practices should maintain a written infection control manual that covers autoclave operation in detail and is reviewed annually. A designated infection control lead — typically a senior dental nurse or practice manager — should be responsible for maintaining documentation, scheduling service visits, and monitoring daily compliance.
A typical Class B cycle including conditioning, sterilization, and drying runs between 25 and 45 minutes depending on the load type and the specific program selected. Fast cycles for unwrapped solid instruments can complete in as little as 15 to 20 minutes on some models. Rapid cassette autoclaves like the Scican Statim can sterilize unwrapped loads in 6 to 9 minutes, making them useful for emergency turnaround situations.
With proper maintenance, a quality dental autoclave should last 10 to 15 years. Replacement is typically warranted when repair costs exceed 50% of a new unit's purchase price, when spare parts become unavailable, when the unit can no longer be certified under current standards, or when software and logging capabilities no longer meet regulatory requirements. Many practices upgrade earlier to take advantage of improved data logging and traceability features.
Many rubber and plastic dental items are autoclavable, but only at appropriate temperature settings and if the material is rated steam-sterilizable by the manufacturer. Items intended for lower-temperature cycles (typically 121°C rather than 134°C) must not be run at higher settings. Always verify the sterilization rating of each instrument type with its manufacturer's instructions for use (IFU) before autoclaving.
Sterility is considered event-related rather than time-related under modern infection control guidelines. This means a correctly packaged, undamaged, properly stored sterile pouch remains sterile indefinitely unless the packaging is compromised — torn, wet, punctured, or exposed to contaminated surfaces. However, many practices implement a practical re-sterilization date (commonly 12 months) as a conservative operational policy. Storage conditions matter: sealed cabinets away from dust, moisture, and traffic are essential.




If you have any question for the installation
or need support, please feel free to contact us.
86-15728040705
86-18957491906
 English
English عربى
عربى