Content
A washer disinfector is a thermally driven automated cleaning and disinfection machine used to decontaminate reusable medical instruments before sterilization. The short answer: it does not sterilize — it cleans and thermally disinfects. Sterilization, including the kind performed by a dental autoclave, comes after. Understanding this distinction is the starting point for any infection control protocol that actually works.
In dental clinics, hospital central sterile supply departments (CSSDs), and surgical centers, the washer disinfector sits at the front of the reprocessing chain. Instruments enter contaminated, pass through enzymatic pre-wash, main wash, thermal disinfection, and drying cycles — emerging clean enough to be safely handled and, where required, loaded into a dental autoclave or other sterilizer. Skip this step, or do it inadequately, and the autoclave cannot do its job: organic soil protects microorganisms from steam penetration.
EN ISO 15883 is the governing standard for washer disinfectors worldwide. It defines performance requirements, test methods, and cycle validation criteria. Compliance with this standard is not optional in regulated healthcare environments — it is the baseline.
Reprocessing reusable instruments follows a defined sequence. Deviation from this sequence compromises patient safety and regulatory compliance. The chain, in order, is:
The dental autoclave is responsible for killing all microbial life, including bacterial spores. But it relies entirely on the washer disinfector having removed organic contamination beforehand. Studies have shown that as little as 6 µm of organic soil can prevent steam from reaching instrument surfaces, rendering autoclave cycles ineffective regardless of temperature and pressure parameters.
This interdependency is why dental practices, oral surgery suites, and hospital dental departments that invest in quality dental autoclave equipment must also ensure their upstream washer disinfector is validated and performing correctly. The chain is only as strong as its weakest link.

A standard washer disinfector cycle consists of several discrete phases, each with specific functional goals. The exact number and naming of phases varies by manufacturer and application, but the core structure is consistent across machines compliant with EN ISO 15883.
Cold or lukewarm water (typically below 45°C) is used in the pre-wash to remove gross contamination — blood, saliva, tissue debris — without coagulating proteins. Hot water at this stage would denature proteins onto instrument surfaces, making subsequent cleaning far more difficult. The pre-wash is a dilution and mechanical flushing step, not a cleaning step.
The main wash phase uses heated water (typically 50–65°C) combined with enzymatic detergents or alkaline/neutral detergents. Enzymatic chemistries break down proteins, lipids, and carbohydrates at a molecular level. The detergent reduces surface tension, allowing cleaning solution to penetrate instrument lumens, joints, and box-lock hinges. Wash temperature, detergent concentration, and cycle time are all validated parameters — changing any one of them without revalidation invalidates the process.
Multiple rinse phases remove detergent residues. Residual detergent left on instruments can interfere with sterilization chemistries and cause tissue irritation in patients. Some washer disinfectors use a neutralizing rinse to balance pH before the thermal disinfection phase.
This is the phase that gives the washer disinfector its disinfection function. Hot water — typically 80°C for 10 minutes, 90°C for 1 minute, or 93°C for 30 seconds — is circulated. These time-temperature combinations are expressed as A0 values under EN ISO 15883. An A0 of 600 (equivalent to 80°C for 10 minutes at z=10) is the standard requirement for disinfection of instruments that contact mucous membranes. This thermal step kills vegetative bacteria, yeasts, molds, and most viruses — but not bacterial spores. For spore elimination, the dental autoclave remains the final necessary step for items classified as critical or semi-critical.
Forced hot air drying — typically at 100–120°C — removes moisture from instrument surfaces and lumens. Adequate drying is critical: wet instruments loaded into a dental autoclave can cause wet packs after sterilization, compromising sterile barrier integrity. Drying also prevents microbial growth during storage between reprocessing and packaging.
Not all washer disinfectors are equivalent. Machine selection depends on instrument volume, types of instruments being processed, available floor space, and workflow requirements. Below is a comparison of the main categories used in dental and healthcare settings.
| Type | Capacity | Typical Application | Key Feature |
|---|---|---|---|
| Countertop / Benchtop | 1–2 trays | Small dental practice, single-chair clinic | Space-efficient; pairs with compact dental autoclave |
| Undercounter / Cabinet | 2–4 trays | Multi-chair dental practice, oral surgery | Integrated into decontamination room cabinetry |
| Freestanding / Pass-Through | 4–20+ trays | Hospital CSSD, large dental hospital | Dirty-to-clean room barrier separation |
| Endoscope Washer Disinfector | 1–6 channels | Endoscopy units, ENT, dental implant scopes | Channel irrigation; chemical disinfection option |
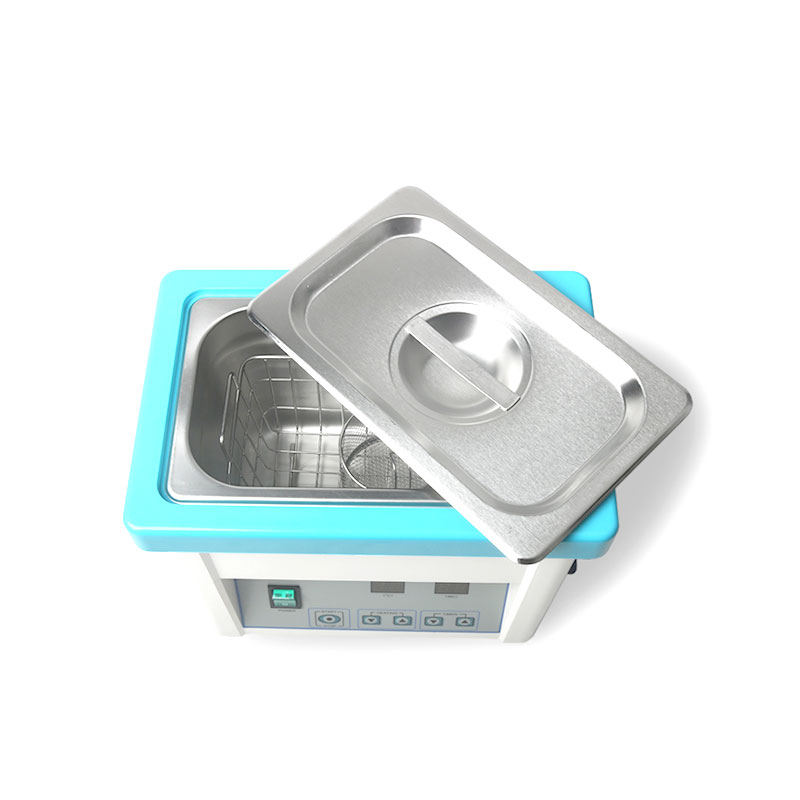
| Ultrasonic + Washer Combo | Varies | Instruments with complex geometry, fine dental burs | Cavitation cleaning + thermal disinfection |
For most general dental practices, a benchtop or undercounter washer disinfector combined with a Class B dental autoclave represents the minimum acceptable standard for processing hollow, lumened, and wrapped instruments. The dental autoclave handles sterilization; the washer disinfector handles everything upstream.
A washer disinfector that has not been validated is not a validated process — it is a machine running a cycle. The distinction matters enormously from a regulatory and patient safety perspective. EN ISO 15883 requires washer disinfectors to undergo Installation Qualification (IQ), Operational Qualification (OQ), and Performance Qualification (PQ) before entering service, mirroring the same framework required for dental autoclave validation under EN 13060.
IQ confirms that the washer disinfector has been installed correctly — water supply pressure and temperature, drainage, electrical connections, and detergent dosing systems are all within specification. This is documented at commissioning.
OQ verifies that the machine performs its cycles correctly under defined conditions — temperature data loggers confirm the thermal disinfection phase reaches and holds the required A0 value, detergent dosing is accurate, and cycle times are correct. OQ is repeated after machine relocation, major repairs, or software updates.
PQ tests cleaning efficacy using standardized test soils (defined in EN ISO 15883-5) applied to representative instruments. A cleaning efficacy index (CEI) test or protein residue test confirms that cleaning is achieving an acceptable standard. PQ must be repeated annually at minimum, and more frequently if instrument types or detergent chemistry changes.
Between formal requalification cycles, daily and periodic monitoring keeps the process under control. Routine tests include:
This monitoring regime mirrors the daily testing required for a dental autoclave — Bowie-Dick tests, vacuum leak tests, and biological indicator monitoring — creating a documented chain of evidence that the entire reprocessing pathway is performing as intended.

A washer disinfector can be perfectly validated, correctly installed, and running a proven cycle — and still produce inadequately cleaned instruments if loading is done incorrectly. Loading is the human variable that validation cannot fully control, and it is the most common source of cleaning failures in practice.
The fundamental principle is that cleaning water and solution must reach every surface of every instrument. This means:
Training and visual loading guides specific to each instrument type should be available at the point of loading. Many CSSD departments laminate loading diagrams and mount them inside the decontamination room. The same rigor should apply in dental decontamination rooms where washer disinfectors feed into dental autoclave sterilization cycles.
Detergent selection is a validation decision, not a purchasing decision. The detergent used during PQ must be the detergent used in daily practice — changing products without revalidation is a compliance failure, even if the replacement appears chemically similar.
High-pH alkaline detergents (pH 9–12) are effective at breaking down proteins and fats. They are the most widely used chemistry in instrument washer disinfectors. However, they can cause accelerated corrosion on aluminum instruments and certain alloys. Dental handpieces, aluminum impression trays, and some legacy instruments may require compatibility testing before alkaline detergents are used.
Enzymatic formulations — typically containing protease, lipase, and amylase — work at lower temperatures and are gentler on delicate instruments. They are particularly effective for protein-heavy contamination common in oral surgery (blood, soft tissue) and are the preferred chemistry for instruments processed alongside complex dental surgical kits destined for a dental autoclave sterilization cycle.
Neutral pH detergents are used for material-sensitive loads. They are less aggressive cleaners than alkaline products and require longer wash times or higher temperatures to compensate. Used in situations where instrument material compatibility is the primary constraint.
Rinse aids reduce water surface tension, improving drainage and reducing water spotting. Instrument protection additives — often containing amine compounds — provide a thin corrosion-protective layer on carbon steel instruments. These are dispensed during the final rinse phase. Over-dosing rinse aid leaves residues that can interfere with steam penetration in the dental autoclave — an often-overlooked cross-phase problem.
Even well-maintained washer disinfectors develop performance problems over time. Recognizing failure patterns early prevents inadequately processed instruments from reaching patients. The following are the most commonly encountered issues and their diagnostic indicators.
| Failure Mode | Likely Cause | Diagnostic Action |
|---|---|---|
| Visible soil remaining on instruments | Overloading, blocked spray arms, inadequate pre-wash | Check spray arm rotation; review loading practice |
| Water spotting / mineral deposits | Hard water, exhausted softener resin, insufficient rinse aid | Test water hardness; check softener salt levels |
| Instruments not drying adequately | Drying element fault, overloaded basket blocking airflow | Check drying temperature; reduce load density |
| Cycle abort / thermal disinfection failure | Heating element fault, cold water inlet issue, sensor failure | Review cycle printout; call service engineer |
| Instrument corrosion / staining | Detergent incompatibility, missing instrument protection additive | Review detergent compatibility data sheets |
| Foam accumulation during cycle | Over-dosing detergent, wrong detergent type, detergent residue from manual washing | Check dosing pump calibration; review pre-cleaning protocols |
Any washer disinfector failure that results in inadequately cleaned instruments must trigger a quarantine of those instruments. They should not proceed to the dental autoclave or any sterilizer — they must be reprocessed from the beginning of the decontamination cycle. Releasing contaminated instruments to sterilization in the hope that the autoclave will compensate is not clinically acceptable and is not supported by any current guidance document.
Regulatory requirements for washer disinfectors vary by country and healthcare setting, but the underlying standards are broadly consistent internationally. Understanding which regulations apply prevents compliance gaps and simplifies procurement decisions.
The primary international standard covering washer disinfectors. Part 1 covers general requirements and definitions. Part 2 covers requirements for machines processing surgical instruments. Part 3 covers endoscope washer disinfectors. Part 4 addresses chemical disinfection of thermolabile endoscopes. Part 5 defines test soils for cleaning efficacy testing. Machines marketed as compliant must meet these requirements, and the certification should be verified at procurement.
In the European Union, washer disinfectors are classified as Class IIa medical devices under MDR 2017/745. This means they require CE marking, conformity assessment by a notified body, and a Declaration of Conformity. The same framework that governs dental autoclave certification applies. Facilities purchasing washer disinfectors for clinical use must verify CE marking status.
HTM 01-05 is the specific guidance for dental decontamination in England and sets out detailed requirements for both washer disinfectors and dental autoclaves used in NHS and private dental practice. It mandates the use of a validated washer disinfector for instruments processed before sterilization in a dental autoclave, specifies the dental autoclave class required (Class B for wrapped and lumened loads), and requires documented evidence of both. Similar guidance documents exist in Scotland (SDCEP), Wales, and Northern Ireland.
In the US, ANSI/AAMI ST79 is the comprehensive guide for sterilization of health care products in health care facilities. It covers automated cleaning and decontamination as prerequisite steps for sterilization and is referenced by the Joint Commission, CMS, and state health departments. FDA 510(k) clearance is required for washer disinfectors sold in the US market.
Manual cleaning of dental instruments — scrubbing with a brush, rinsing under running water — was the standard for decades. It remains in use in settings without washer disinfectors, but the evidence for its inferiority to automated cleaning is substantial and consistent.
A study published in the Journal of Hospital Infection found that automated washer disinfector processing reduced protein contamination on surgical instruments by 99.5% compared to manual cleaning, which reduced contamination by approximately 84% under the same conditions. The gap is explained by two factors: consistency and physics.
Manual cleaning is inherently variable. Different operators apply different pressure, use different brush technique, and spend different amounts of time on each instrument. A box-lock hinge cleaned thoroughly by one technician may be inadequately cleaned by another. Automated washer disinfector cycles, once validated, apply the same mechanical action, temperature, chemical concentration, and time to every load, every time.
Manual cleaning also exposes staff to contaminated sharps. Dental instruments — scalers, curettes, surgical burs, extraction forceps — represent a real sharps injury risk during manual handling. Washer disinfectors eliminate this exposure for the cleaning phase. After thermal disinfection, instruments can be handled with standard gloves rather than the heavy-duty puncture-resistant gloves required for contaminated sharps.
The dental autoclave at the end of the reprocessing chain performs best when fed by a consistent, validated cleaning process. A washer disinfector provides that consistency in a way that manual cleaning structurally cannot.
Preventive maintenance is not optional — it is the mechanism by which validated performance is maintained between qualification cycles. The following table summarizes a standard maintenance schedule applicable to most washer disinfector models.
| Frequency | Task | Responsibility |
|---|---|---|
| Daily | Check spray arm rotation; clean filter screens; verify detergent/rinse aid levels; review cycle printout | Operator |
| Weekly | Clean door seals and gaskets; inspect wash chamber walls for debris buildup; check detergent dosing pump output | Operator |
| Monthly | Water hardness test; conductivity check on final rinse water; inspect door hinge and latch mechanisms | Operator / Supervisor |
| Quarterly | Protein residue spot check on processed instruments; calibration check of temperature sensors | Supervisor / Engineer |
| Annually | Full requalification (OQ/PQ); service engineer inspection; replace filters and worn parts per manufacturer schedule | Service Engineer |
Annual service visits should be scheduled with an authorized service engineer, not deferred when the machine appears to be functioning normally. Heating elements, door seals, detergent pumps, and water softener resin all degrade over time in ways that do not produce immediately visible cycle failures but do result in reduced cleaning efficacy.
Designing a functional decontamination room — or upgrading an existing one — requires thinking about the washer disinfector and dental autoclave as a system, not as two independent purchases. The physical workflow, spatial layout, and staff movement should all support a dirty-to-clean unidirectional flow: contaminated instruments in, sterile instruments out, with no backflow of contaminated materials into the clean zone.
Key design principles for a compliant dental decontamination room include:
In new-build dental practices, decontamination room design should be completed before construction begins, with input from the dental autoclave and washer disinfector suppliers regarding plumbing, drainage, electrical, and ventilation requirements. Retrofitting a decontamination room into an existing space is possible but often requires compromises that reduce workflow efficiency.
No. A washer disinfector achieves thermal disinfection — it kills vegetative bacteria, fungi, and most viruses — but it does not achieve sterilization. Bacterial spores survive the thermal disinfection phase. For instruments classified as critical (those that penetrate tissue or bone) or semi-critical (those that contact mucous membranes and cannot be single-use), sterilization in a dental autoclave is required after washer disinfector processing. The two machines perform different functions and neither can substitute for the other.
Only if the handpiece manufacturer explicitly states that the specific model is washer-disinfector-compatible. Many turbines and contra-angles are damaged by immersion in water or exposure to the temperatures involved. Compatibility must be checked against the manufacturer's Instructions for Use (IFU) for both the handpiece and the washer disinfector. Non-compatible handpieces are processed using appropriate handpiece maintenance equipment and then sterilized in a dental autoclave according to the handpiece IFU.
Cycle times vary significantly by machine model, cycle type, and load. Typical cycles for dental instrument sets run between 25 and 60 minutes from start to end of drying. Some machines offer express cycles of 18–22 minutes for lightly soiled loads, but these shorter cycles must be validated for the specific instruments and contamination types involved. Rushing cycle times without validation is a compliance breach, not a workflow optimization.
Yes, without exception. Dental autoclave validation confirms that the sterilization step works on clean instruments. It does not validate or compensate for inadequate cleaning. Regulatory guidance — including HTM 01-05 in the UK, EN ISO 15883, and ANSI/AAMI ST79 in the US — requires washer disinfectors to be independently validated. Both machines require their own documented qualification, and both must be maintained within their validated parameters.
Any instrument load from an aborted or incomplete cycle must be treated as contaminated and reprocessed from the beginning. Do not load it into the dental autoclave. Check the cycle printout or machine log to identify the phase at which the cycle failed, note the error code, and contact the service engineer. Instruments from aborted loads should be re-soaked in enzyme solution to prevent biofilm formation during the period before reprocessing begins.
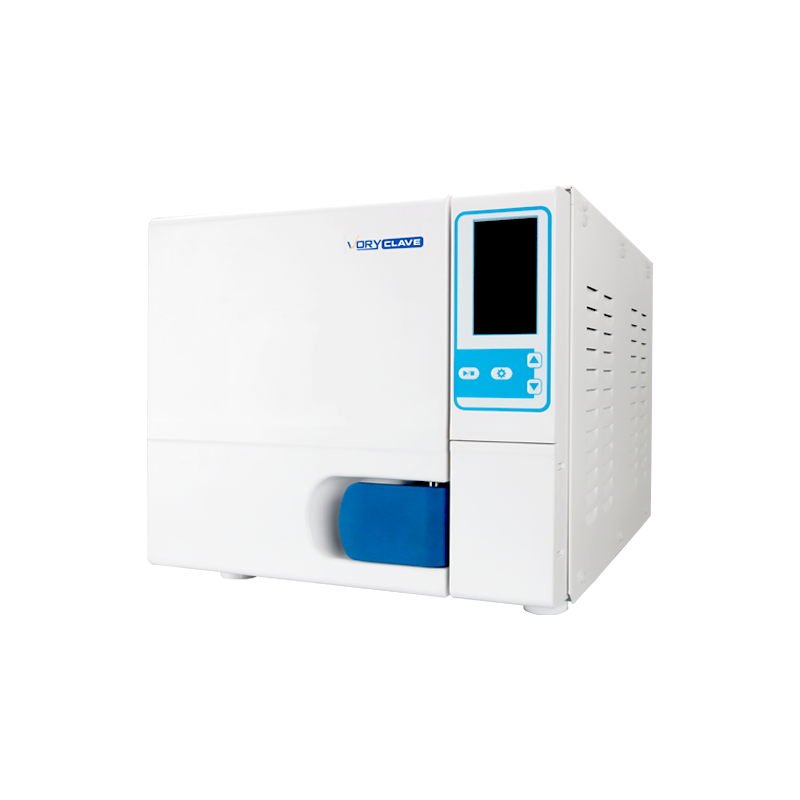
A Class N dental autoclave (often incorrectly referred to as Class A in older literature) is suitable only for solid, unwrapped instruments. A Class B dental autoclave uses a pre-vacuum cycle to remove air from instrument lumens and porous materials before steam penetration, making it the only appropriate type for wrapped, hollow, or porous loads. Instruments exiting a washer disinfector that are destined for wrapped sterile storage or that include hollow lumens must be processed in a Class B dental autoclave — not a Class N or Class S machine.






If you have any question for the installation
or need support, please feel free to contact us.
86-15728040705
86-18957491906
 English
English عربى
عربى